Ocular pentastomiasis is an exceptionally rare yet profoundly serious zoonotic infection that can lead to irreversible vision loss.
Caused by the larval stage of pentastomids—also called tongue worms—this condition highlights the hidden dangers of certain parasitic arthropods that bridge the evolutionary gap between crustaceans and worms.
While most human infections remain asymptomatic in visceral tissues, ocular involvement produces dramatic symptoms because the eye’s delicate structures cannot tolerate even minor invasion.
Pentastomids such as Armillifer armillatus and Linguatula serrata are the primary culprits. Adult parasites live in the respiratory tracts of definitive hosts—snakes for Armillifer species and canids like dogs for Linguatula.
Humans become accidental intermediate hosts after ingesting infective eggs, often through contaminated water, unwashed hands, or undercooked bushmeat.
Once hatched, larvae penetrate the intestinal wall and migrate systemically.

Transmission is closely linked to cultural practices and poor sanitation in endemic areas, particularly Central and West Africa.
Consumption of snake meat or close contact with infected reptiles increases exposure risk.
Larvae encyst in many organs but occasionally continue migrating to the eye, where they cause localized destruction.
This pathway explains why ocular cases, though uncommon, are more readily diagnosed than visceral ones.
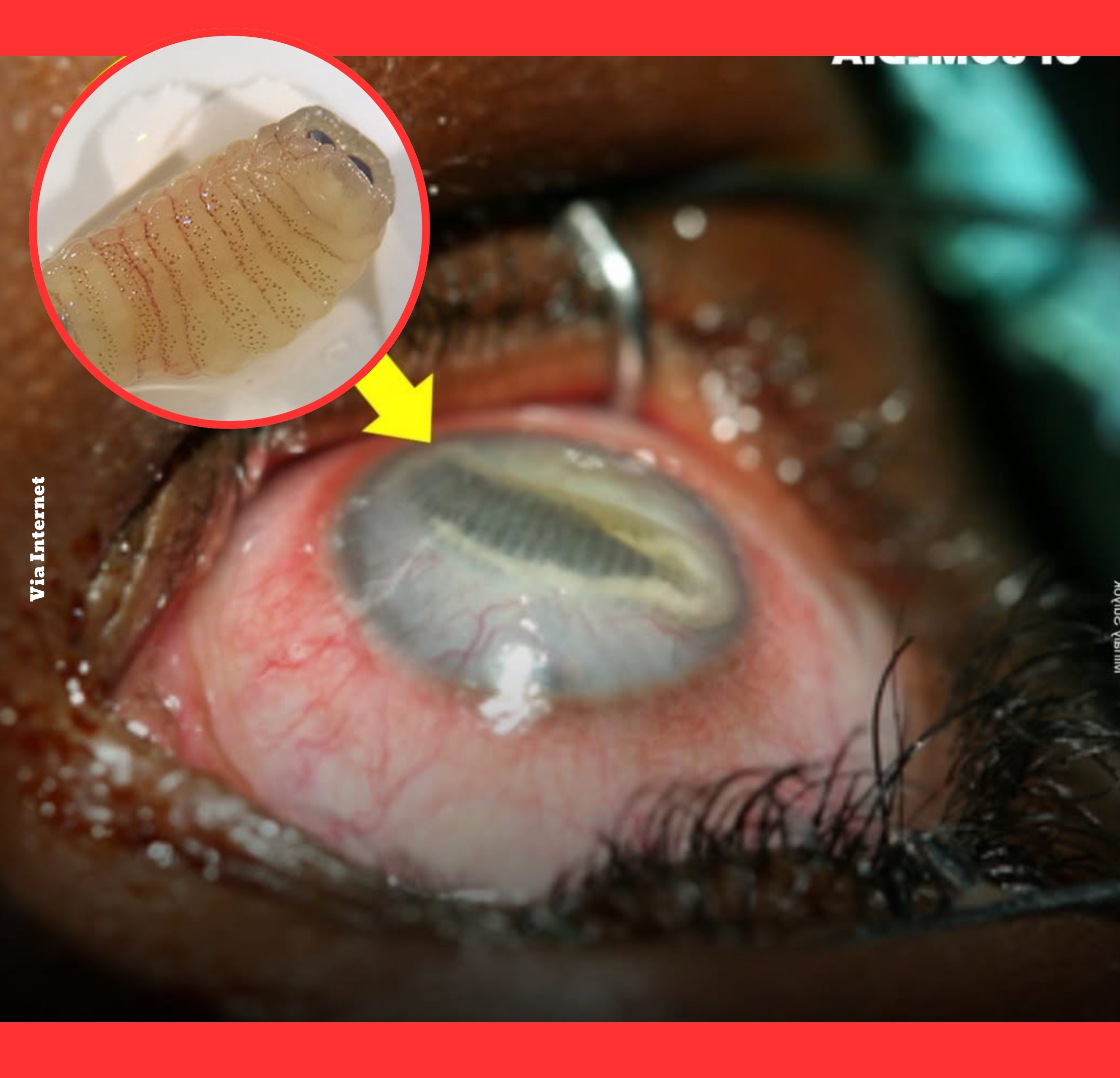
In the eye, larvae typically settle in the anterior chamber, subconjunctival space, or posterior segment.
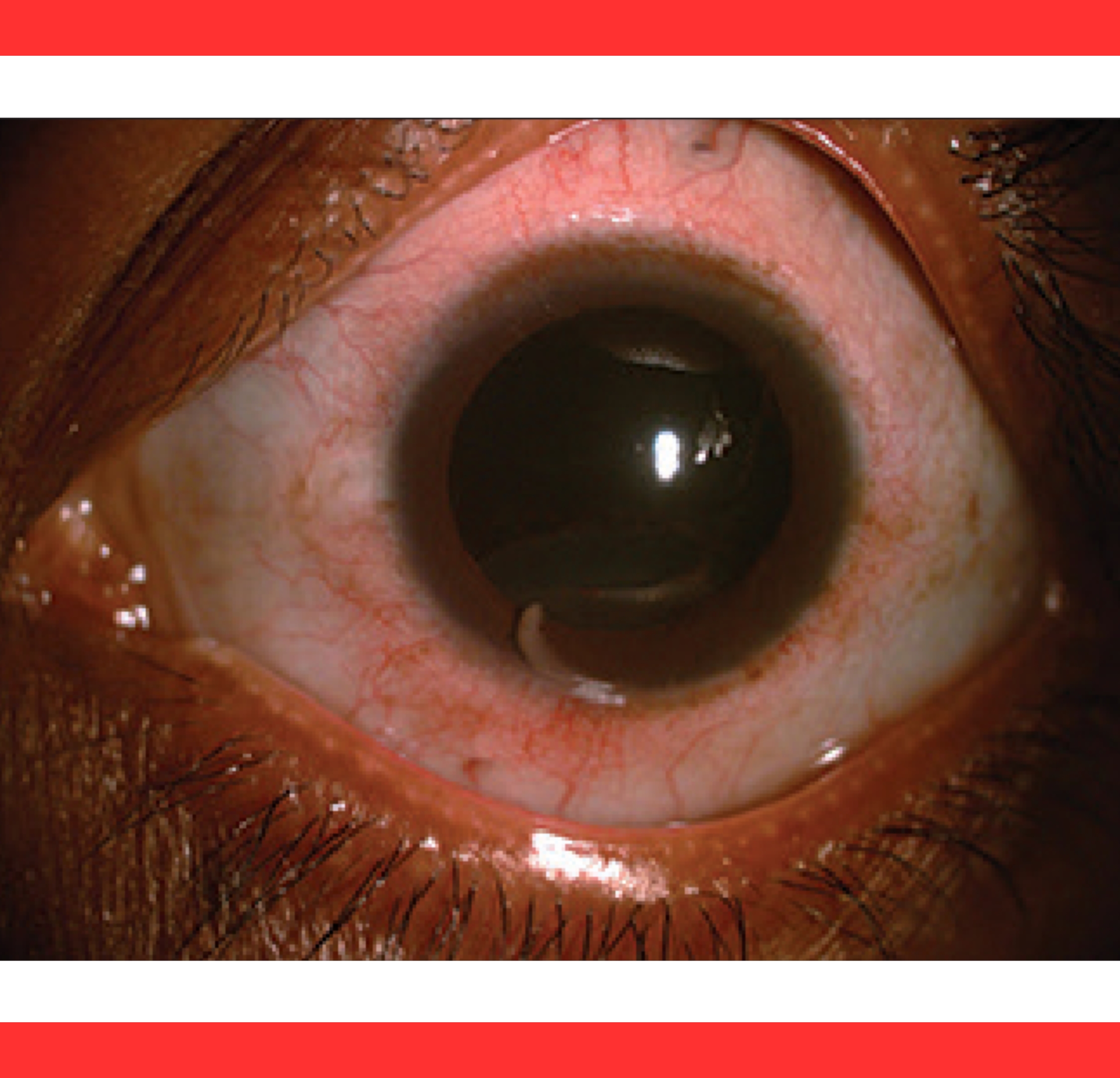
Their movement and growth provoke intense inflammation, mechanical trauma, and secondary complications including iritis and glaucoma.
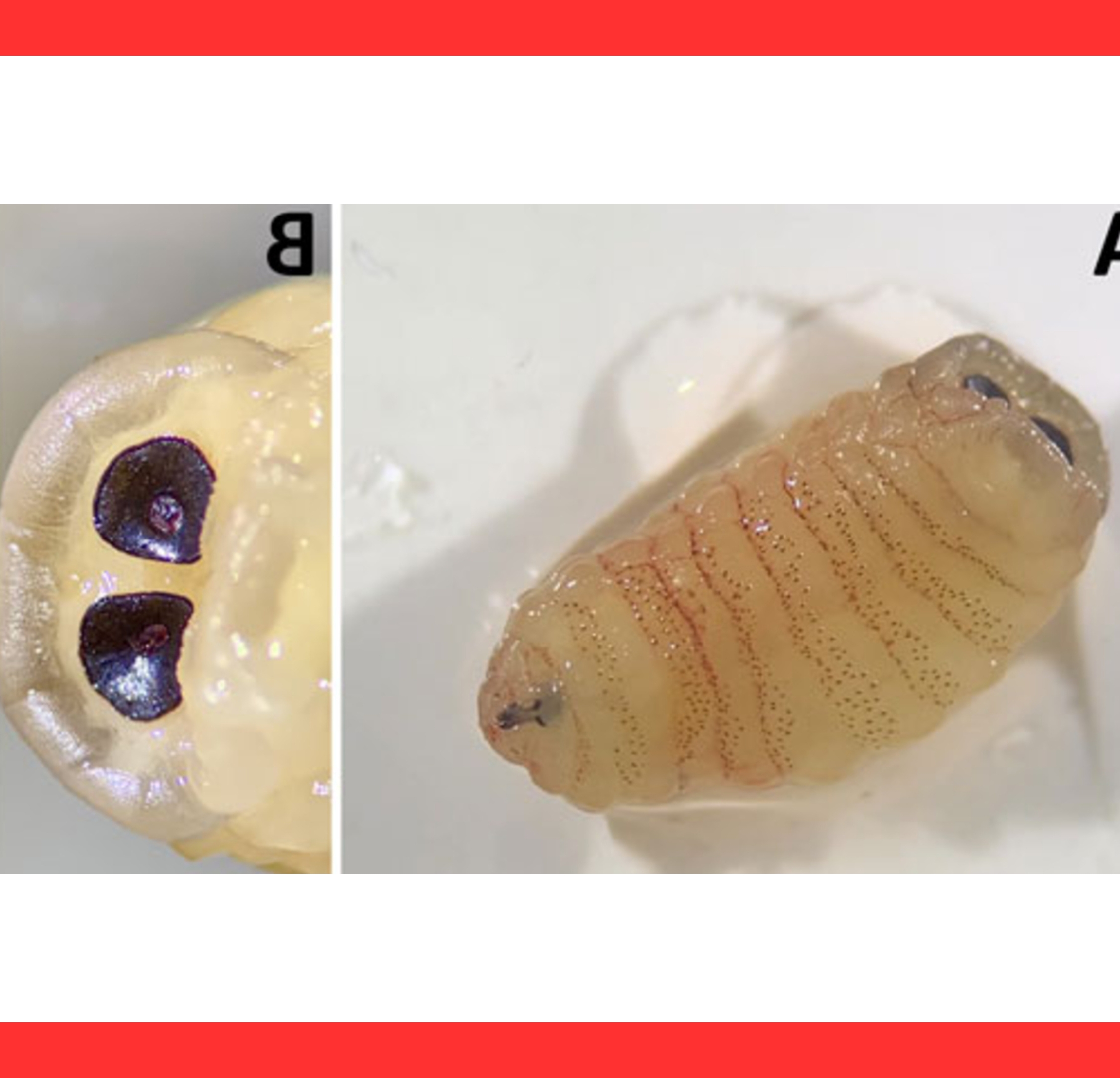
The parasites appear as glistening, annulated, C-shaped bodies that exhibit visible peristalsis under slit-lamp examination, alerting clinicians immediately.

Patients report acute eye pain, conjunctival redness (hyperemia), photophobia, and rapidly worsening vision.
In advanced cases, the larva’s presence can cause corneal edema, hyphema, or retinal damage, culminating in complete blindness.
Symptoms are usually unilateral but can be bilateral if multiple larvae migrate. Early recognition is critical because delays allow irreversible scarring.
Diagnosis combines clinical observation with surgical confirmation.

Physicians often spot the moving parasite directly; microscopic examination of the extracted specimen reveals characteristic hooks and annulations that distinguish pentastomids from other eye worms.
Imaging and laboratory tests help rule out mimics such as cysticercosis or loiasis.
Surgical extraction remains the cornerstone of treatment.
Surgeons remove the larva as quickly as possible to halt ongoing inflammation and prevent further tissue damage.
Adjunctive corticosteroids control swelling, while antiparasitic drugs offer limited benefit once the organism has reached the eye. Supportive care addresses secondary glaucoma or infection.
Prognosis depends on timely intervention.
Reported series show permanent visual acuity reduction in roughly 69 percent of intraocular cases and total vision loss in 31 percent.
Factors worsening outcomes include delayed surgery, larval location near the optic nerve, and host inflammatory response.
Visceral pentastomiasis is often incidental, but ocular disease is devastating.
Prevention hinges on education and hygiene.
Communities in high-risk zones should avoid raw reptile or canine meat, boil drinking water, and wash hands after animal contact.
Public health programs promoting safe food practices and awareness of bushmeat risks can reduce incidence.
Travelers to endemic regions should exercise caution with local cuisine.

Ongoing research into pentastomiasis remains limited due to its rarity, yet climate change and expanding bushmeat trade may increase future cases.
Greater awareness among ophthalmologists and primary-care providers in tropical settings could improve early detection and save sight.
International collaboration is essential to document and control this cryptic parasite.
Ultimately, ocular pentastomiasis serves as a stark reminder of humanity’s vulnerability to zoonotic threats.
Simple behavioral changes and prompt medical attention offer the best defense against a parasite capable of robbing patients of their vision forever.
Continued vigilance and research will be key to protecting vulnerable populations from this silent ocular invader.