Medical professionals are raising awareness about a rare yet potentially life-threatening phenomenon where respiratory infections and certain lung diseases lead to the creation of unusual jelly-like structures in the airways.
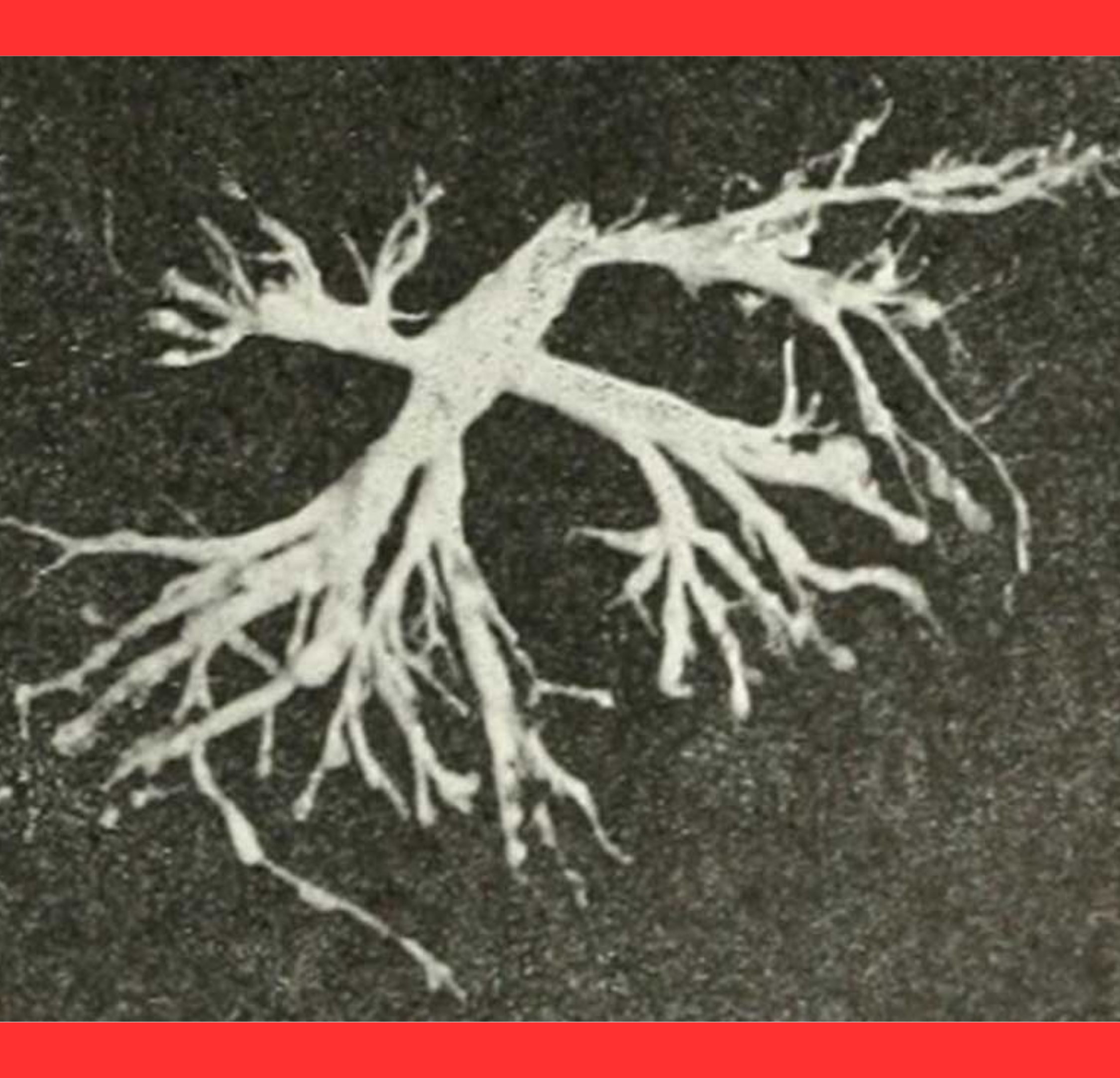
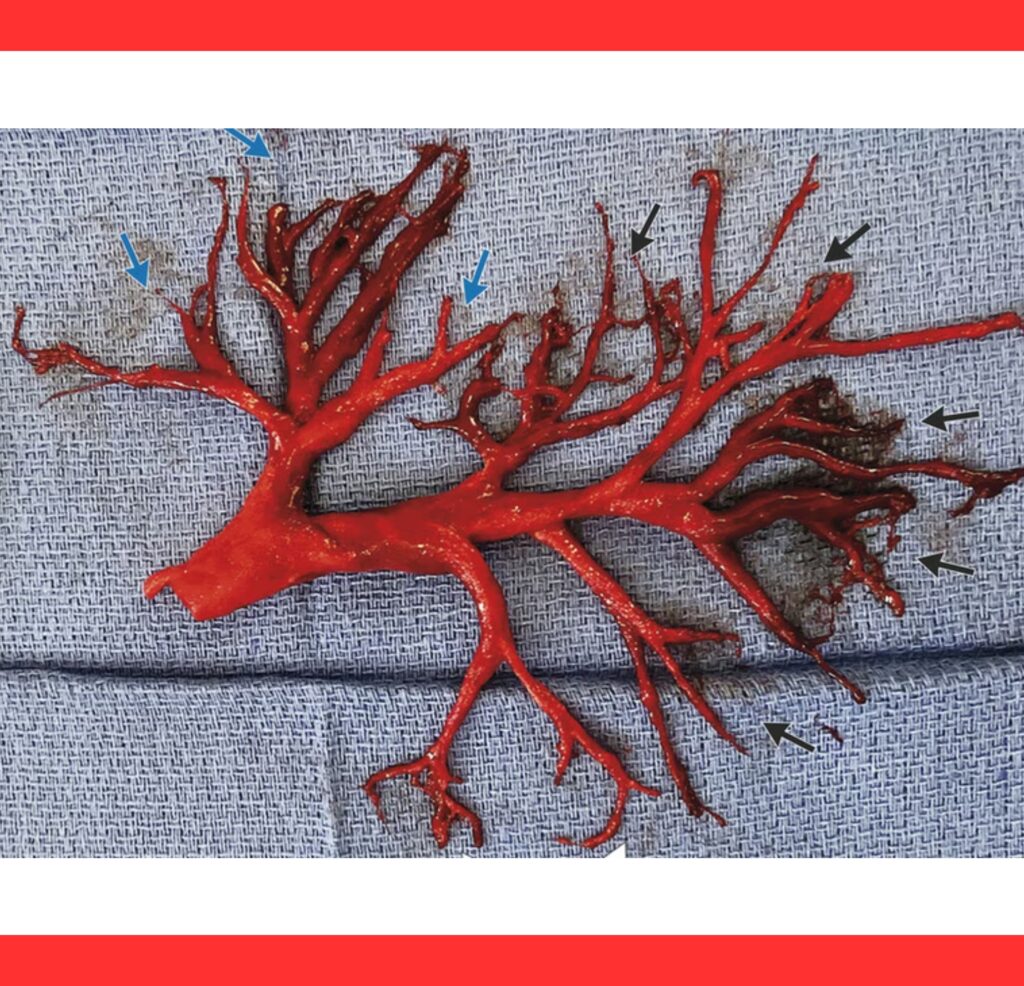
These bronchial molds, often referred to as casts, can form intricate replicas of the lung’s branching tubes, severely impeding normal breathing.

Known medically as plastic bronchitis, the condition involves the accumulation of materials that solidify within the bronchi, forming rubbery plugs.
Patients have reported coughing up these casts, which sometimes resemble miniature trees or the exact anatomical mold of their respiratory passages.
The casts are typically composed of thick mucus mixed with fibrin, inflammatory cells, and in some cases, lymphatic fluid that leaks abnormally into the airways.
When exposed to air, this fluid can gel and harden, creating obstructive barriers.
Respiratory infections such as severe bacterial pneumonia, viral illnesses including influenza or COVID-19 complications, and chronic conditions like asthma or allergic bronchopulmonary aspergillosis (ABPA) are common triggers.
These diseases promote excessive mucus production and inflammation that contribute to cast formation.
In other instances, particularly among children who have undergone heart surgeries like the Fontan procedure, faulty lymphatic drainage systems allow protein-rich lymph to enter the lungs, solidifying into casts.
Symptoms often begin with persistent coughing and difficulty breathing, progressing to wheezing, chest pain, and oxygen deprivation if the molds block major airways.
In extreme cases, they can cause complete lung collapse or respiratory failure.
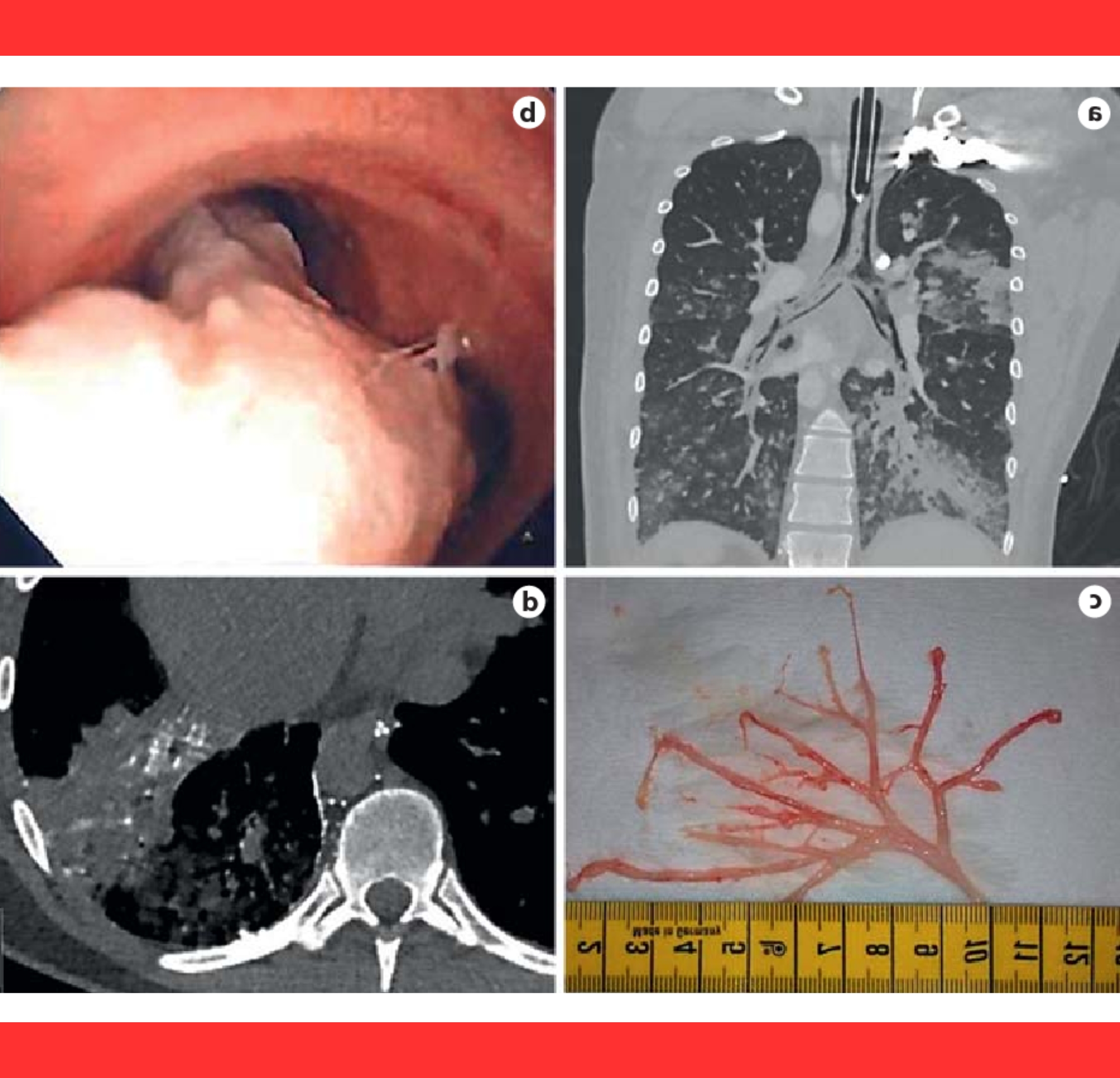
Diagnosis is confirmed when patients expectorate the casts or through bronchoscopy, where doctors directly visualize and extract the molds.
Imaging techniques like CT scans may also reveal the characteristic filling of the bronchial tree.
Treatment strategies include urgent removal of the obstructing casts using bronchoscopic tools to restore airflow.
Addressing the underlying infection or disease is crucial, often involving antibiotics, anti-inflammatory drugs, or specialized lymphatic therapies.
Healthcare providers emphasize early intervention, as recurrent cast formation can lead to repeated hospitalizations and long-term lung damage.
Supportive care such as humidified oxygen and chest physiotherapy may aid in management.

Researchers are investigating new approaches, including medications that alter mucus properties or procedures to correct lymphatic abnormalities, offering hope for better control of this distressing condition.
As respiratory illnesses continue to circulate globally, understanding and recognizing signs of bronchial mold formation could prove vital in preventing severe complications and saving lives.
Patients experiencing unusual symptoms are advised to consult specialists promptly.